The patient journey project: Workshops
A series of national events designed to help people suffering with Glioblastoma and their carers to “Be the Captain Of Your Cancer”. This uses a holistic approach which empowers you to better manage your new life.
 These workshops are supplementary to our fatigue, communication and carer workshops and have been designed in partnership with Pablo Lievano and Greg Gerard. Pablo and Greg have both been living with Glioblastoma, and their determination and passion to help improve the lives of others walking this road is unparalleled. Sadly Pablo passed away recently, but the events continue as part of an incredible legacy to help others living with this disease.
These workshops are supplementary to our fatigue, communication and carer workshops and have been designed in partnership with Pablo Lievano and Greg Gerard. Pablo and Greg have both been living with Glioblastoma, and their determination and passion to help improve the lives of others walking this road is unparalleled. Sadly Pablo passed away recently, but the events continue as part of an incredible legacy to help others living with this disease.
These events are kindly supported by:

Past workshops
Clinician and patient workshop October 2018
Hosted with the support of Cliveden House Hotel, this event brought together clinicians, patients, caregivers and supportive organisations to identify the gaps in the Glioblastoma patient journey. The event was well attended and outcomes vital in informing the work of the professionals and volunteers that came along.

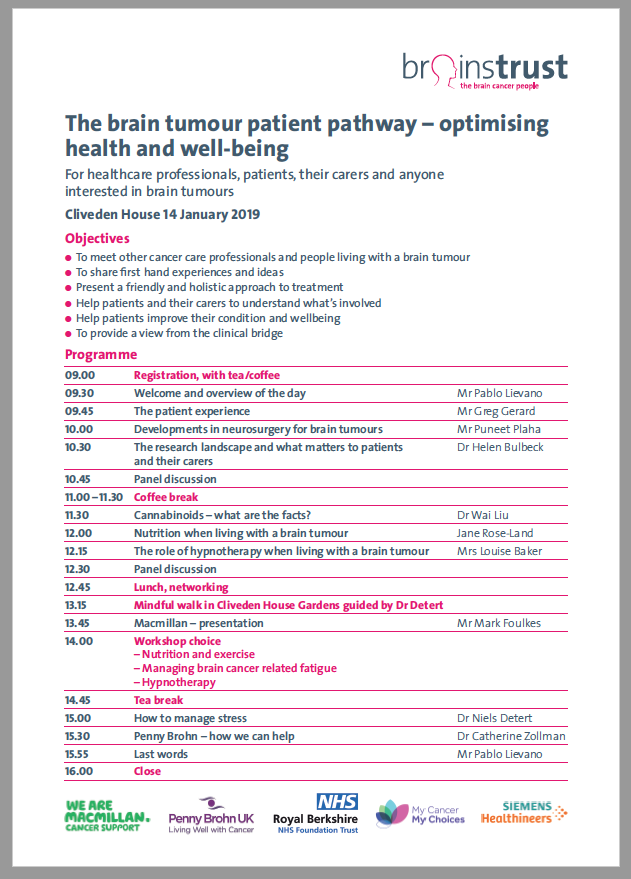
Cliveden House January 2019
This event, attended by 50 patients and caregivers had a broad programme that included patient experience, developments in neurosurgery, cannabinoids, managing stress and nutrition.

Health and Well-being workshop July 2019
- Northwest Biotherapeutics about the role that immunotherapy has in treating glioblastoma. More information can be found in the Know How
- Mr Plaha, our insightful consultant neurosurgeon, on the latest advances in first line treatment – brain surgery.
- Experts in diet and nutrition, mindfulness, hypnotherapy and complementary therapies, who led various workshops throughout the day.

Upcoming workshops
These events to help people living with Glioblastoma are being expanded across the UK. Full information and registration will be via www.meetup.com/brainstrust. At the moment we are looking to run events in the following regions:
Stay tuned to find out when events will be happening near you.
Example programme
Click the image below to see the programme for a typical workshop.