Our impact – getting it right.
“Adding rigour to reporting beyond simply counting beneficiaries is an open goal for charities. We owe it to all of our supporters to be doing an incredible job at communicating the difference our work makes.” – Will Jones, Chief Executive, brainstrust

Impact Report
It is important you know what we have achieved, as well as where we might be falling short. Your stories and feedback have always been steered our work, and we have been working hard in recent years to develop processes that make us best in field at sharing what you are helping us to achieve. That’s why we commit to sharing the annual impact of our work at brainstrust.
Click here to download our latest impact report.
Annual Reports and Accounts

For a more detailed breakdown of our impact, you can download our most recent Trustee’s Annual report and Accounts here.
What we look at.
We report on people’s progress against six indictors, all of which support the four priorities in our strategy. These six indicators are:
- engagement with care and condition
- reduced isolation
- engagement with communities
- creating control
- feeling supported
- feeling resourced
“The help and support has been fantastic so far and came just at the right time. I am starting to find my feet again and thankful to have such a great connection of support through brainstrust” – Patient
Our impact in 2024/2025
This figure shows the progress that beneficiaries who have come to us in the last year (April 1st, 2024, to March 31st, 2025) have made in the last year across the 6 key strategic indicators.
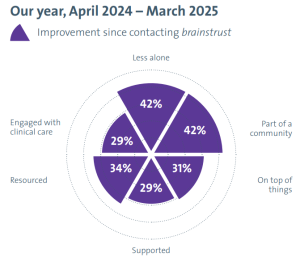
• We helped people improve the most with feeling part of a community and feeling less alone, where both saw a 42% increase.
• After that, we saw an increase of 34% with helping people to feel resourced.
• An area our focus would be helping people to feel engaged with clinical care, where we saw our smallest increase of 29%.
Focuses for the future
While we are still having a positive impact and improving well-being across all six indicators, we have work to do to ensure those who would benefit from our support are able to access us when they need it most. This reinforces the need for strong clinical engagement and making sure brainstrust is accessible, available and a known option for all patients at every point of their pathway.

Our impact reports
Since we embarked on our new strategy, we began to publish impact reports annually to share our progress. You can download these here.





‘None of us is as smart as all of us’
Meaningful collaboration and co-creation is a key component of our approach as we work to secure the best outcomes for anyone who is living with a brain tumour. Partnerships are an essential part of how we create this impact. Find out more about the partnerships and collaborations that are vital to our work.
Join our mission
Help brainstrust continue to have an impact by becoming a regular donor. From as little as £3 a month you can help ensure out vital services can continue to be there for people who are afraid and alone after a brain tumour diagnosis.







