How we raise the money needed to support people with a brain tumour
“Our supporters continue to inspire us with their ideas for fundraising activities, and it’s rewarding to be able to take a tailored and individualised approach to the way we help to realise their ambitions and passions.” – Julia Smith, fundraising manager at brainstrust
In 2024 our supporters raised £652,450 to fund brainstrust’s mission. This income remains from a diversified mix of traditional charity fundraising activity. Our funding comes from:
- Direct and regular giving from supporters
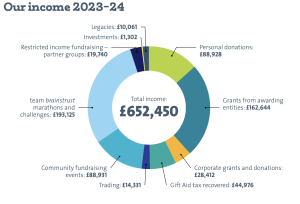
- Fundraising at home and in the community
- Sponsored events and challenges taken on by our incredible community
- Companies who support our work
- Other charities in the form of grants from trusts and foundations
- Gift Aid recovery
- In memory giving
- Trading
We have very limited income from special purpose fundraising, legacy fundraising and high-net-worth individuals and no investment income.
Fundraising headlines and highlights in recent times include:

Ravi’s Dream
Ravi Adelekan has been raising funds for both brainstrust and the brain tumour charity since he was diagnosed with a brain tumour. He continues to be a beacon of inspiration for the brain tumour community, and has raised an incredible £100,000 in 2024!
European challenges played a big part in the fundraising success for 2024, with Team Brainstrust runners taking on the Barcelona Marathon, Paris Marathon and Amsterdam Half and Marathon. Across these events, 28 Team Brainstrust superheroes helped raise an amazing £25k for the charity. Special mentions must go to Ryan Doyle who took on Barcelona Marathon in support of his best friend who is battling a brain tumour who raised £3k and Rob Gower who smashed the Paris Marathon and raised over £3k in memory of his grandad.

Follow The Seagulls saw 34 keen hikers taking on either 26 miles in 1 day or 50 miles over 2 days in challenges at Whitby, on the Isle of Wight, in Fife and in Dartmouth to support the brain tumour community. Not only did all complete the challenge but they also raised over £31k for brainstrust.


Brainstrust Bass Belle 10k, a new portfolio event for brainstrust was held for the first time in June and proved a popular race for young and old. The event sold out which is unusual for new events and raised over £12k for brainstrust. The brainstrust Bass Belle 10 miler was held for a 10th time in 2024 and like the 10k, sold out in record time and raised around £20k.

2024 also showed that running could be fun with a group of 7 Team Brainstrust runners not only taking on Run Thorpe Park 10k but then also facing their fears on some of the rides at the park including ‘Saw’ and ‘Stealth’. Over £5k was raised by Team Brainstrust runners at Run Thorpe Park,

Support from trusts and foundations
A very big thank you to our trust and foundation partners for caring about people who are living with a brain tumour diagnosis. Your support has played a meaningful role in helping brainstrust to survive and thrive. Your compassion has helped us to make a difference to patients and caregivers living with a life-changing diagnosis.
We are an Edward Gosling Foundation legacy partner whose generous support has assured our long term future. Thank you also to The National Lottery and players of The National Lottery who are helping us reach patients and caregivers in all four nations of the UK.
We are grateful to the very many trusts and foundations for their long standing support for brainstrust over the years.
If you’d like to support our work, please do get in touch. Email hello@brainstrust.org.uk or call 01983 292405.